Introduction
Since being trained as an aromatherapist over 24+ years ago aromatherapy has grown tremendously in the field of esthetics/skin care. Research into the therapeutic benefits of applying essential oils to the skin have been able to prove that essential oils offer a wide range of activity for a variety of skin conditions. Essential oils are able to reduce inflammation, enhance wound healing, treat fungal, bacterial, and viral infections, relieve itching, prevent wrinkles and slow the aging process, support the detoxification process, and serve as penetration enhancers for allopathic medicines. With such a vast array of therapeutic benefits, it is no wonder that aromatherapy is growing in popularity within the cosmetics and esthetics industries as well as with individual consumers seeking more natural means of maintaining and supporting the health not only of the skin but of their whole body.
According to Harris, “treating skin diseases and promoting and maintaining skin health is of worldwide relevance and represents a multi-billion dollar market to the pharmaceutical, fragrance, cosmetics and toiletries industries. Aromatherapists have at their disposal remarkable tools that can simply and positively impact a range of commonly encountered skin conditions responsible for significant psychosocial distress. The aromatherapist is able to work at the level of the cutaneous interface not only through the judicious application of essential oils and their related products, but also through touch, olfaction and stress reduction with their subsequent positive impacts on skin health”.1
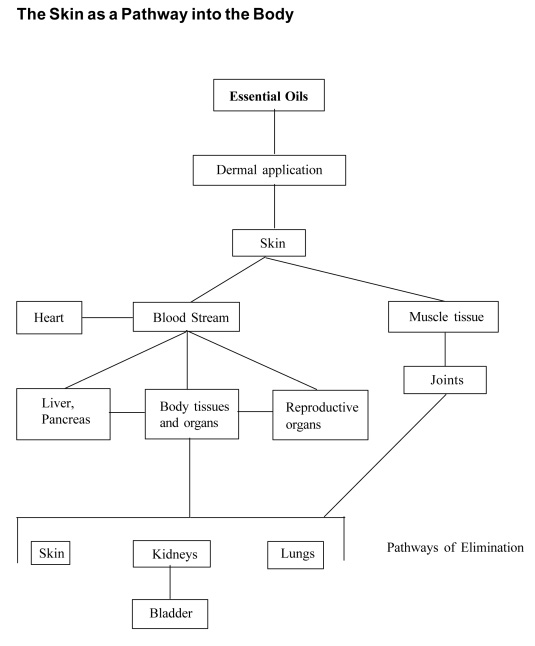
The Skin as a Pathway onto and into the Body
With an understanding of the anatomy and physiology of the skin we will now explore the skin as a pathway onto and into the body. The popular application of essential oils to the skin has been contributed to the seminal work of Marguerite Maury entitled: Marguerite Maury’s Guide to Aromatherapy: The Secret of Life and Youth, published in France in 1961. In her book Maury quotes Dr. Badmadjeff as saying “If it is possible to influence an individual from the outside to the point of modifying his philosophy, it must be done by means of aromatic substances – and through the skin”.2
During her career Maury sought and found, via dermal application, a method of application for essential oils which was capable both of influencing the muscular tonus, the quality and aspect of the skin and the tissues, and to obtain a better functioning and a normalization of the individual’s rhythm.3 Maury was able to successfully merge aromatherapy with hands-on applications (bodywork and skincare).
In 1992 Tony Balacs wrote “Aromatherapists tend to believe that the recipients of aromatherapy massage will gain benefit in three ways: from absorbing the essential oil through the skin, from inhaling the vapor, and from the massage itself”.4 And indeed, this statement holds true today. The skin is a pathway onto and into the body whereby essential oils exert their influence on the skin itself as well as a pathway into the body where essential oils enter general blood circulation possibly influencing the whole health of the body.
The skin is highly efficient at transporting small, relatively fat-soluble molecules like essential oils into the body’s interior, especially when aided by a circulation-stimulating massage.5
Factors which affect the degree to which essential oils are absorbed into the skin include:
- Temperature of the skin
Skin which has been warmed through bathing or the application of a compress tends to be more permeable than cold skin. - Hydration of the skin
Skin exhibiting good hydration tends to be more permeable than dehydrated skin. - Lipophilic nature & molecular structure
Essential oils are known to be highly lipophilic, which means they are attracted to fat. Essential oils are also known to have a small molecular structure which enables them to permeate through the stratum corneum into the dermal layer and on into systemic blood circulation. - Skin integrity
The condition of the skin has an affect on the permeability of essential oils. Damaged or compromised skin is often more permeable than healthy skin. Bensouilah and Buck note that skin diseased by a transient infection or a chronic condition such as psoriasis or dermatitis, in general is more permeable than healthy, normal skin. “A notable exception occurs when the skin becomes thickened or lichenified”.6 (Lichenified means the skin has become thickened and leathery. This often results from continuous rubbing or scratching on an area of skin. Chronic irritation due to conditions such as eczema can cause lichenified skin. http://www.nlm.nih.gov/medlineplus/ency/article/003251.htm) Caution should be used in dosage and choice of essential oils for treatment of damaged or compromised skin conditions. - Hair follicles and thickness of skin
It has long been assumed that one of the entrance pathways for essential oils is through the hair follicles. Areas with a greater number of hair follicles may allow increased essential oil penetration and absorption.
Pugliese points at that “the pores of the sebaceous and sudoriferous glands act as openings onto the skin from which pour out sweat and various oils. Pores also act as channels, carrying substances placed on the skin down into the deeper dermal layers of the skin”. Therefore “skin covered with hair can absorb more applied material than hairless skin”.7 He further notes that the sweat glands are located all over the body, but are more numerous in the palms of the hands and in the soles of the feet. “The sweat glands are openings to the dermis and a potential systemic route of delivery for topically applied products”.8
NOTE: The above information offers a valuable understanding as to why many aromatherapists recommend dermal application of essential oils to the feet. Not only do the feet allow for dermal penetration of essential oils but each foot has over 7000 nerve endings and hence essential oils may also exert an affect on the nervous system.
- Occlusion
Occlusion refers to the process of applying essential oils and then covering them with something like a body wrap or compress. This occlusion will allow for greater penetration of essential oils. - Other factors which affect dermal permeation of essential oils include: humidity levels, duration of contact with substance, higher dosages, and the delivery system utilized to carry the essential oils onto the skin.
Once essential oils have been absorbed through the skin, they are able to affect the skin, muscles and joints as well as body tissue and organs. Bowles writes “It is not known to what extent essential oil constituents penetrate to the adipose layer from a dermal application, though dermally applied oils do appear to have anti-inflammatory and analgesic effects on muscles and joints without having to enter the systemic circulation”.9
Essential oils are then excreted in the urine, feces, perspiration and breath. According to Cooksley, essential oils take 15 minutes to 12 hours to be fully absorbed and about 3 to 6 hours to be expelled in a normal healthy body.10 Absorption and excretion times increase for individuals with obesity or who have poor circulation, or thickened skin. With regards to absorption, not all components of an essential oil are absorbed equally; rather some constituents penetrate more quickly than others. As Buckle points out, in the case of lavender, most of the two main constituents, linalol and linalyl acetate, were absorbed within 20 minutes and eliminated within 90 minutes.11
Buckle further comments that the study of where essential oils go when they are absorbed and how they are absorbed and eliminated by the body is still not fully understood.12 What is known is that essential oils exert a profound influence on overall well-being when used correctly.
The application of essential oils onto and into the skin can offer the following therapeutic benefits:
- Reduce topical inflammation
- Support the regulation of sebum production
- Aid the process of detoxification in the skin
- Increase local circulation
- Support the improvement of muscle tone
- Relax and soothe muscles and joints
- Reduce muscle spasms
- Relieve nerve pain
- Reduce dermal and muscular inflammation
- Provide a cooling or warming affect
- Serve as antioxidants, protect the skin from free radical damage
- Support health of the skin
- Provide antibacterial, antifungal or antiviral activity
- Support healthy lymphatic flow
- Relax and soothe the nervous system
- Provide specific therapeutic benefits for common skin conditions
- Aid in the treatment of sprains, strains, and repetitive movement injuries
- Encourage cellular regeneration, thus making essential oils effective remedies for wound healing and possibly slowing the aging process
- Support and enhance immune cells of the skin, encouraging the whole immune system via the Langerhans cells
- Support wound healing
- Provide valuable emotional support
- Relieve stress and anxiety which may either be causing or be a reaction to a skin condition
Essential oils as novel skin penetration enhancers
There is increasing interest in essential oils as novel dermal penetration enhancers by the pharmaceutical industry. Transdermal drug delivery is defined as the controlled release of drugs through intact and/or altered skin to obtain therapeutic levels of a drug systematically and to affect specified targets for the purpose of, for example, blood pressure control, pain management, and others. The advantages of transdermal drug delivery include: bypassing gastrointestinal incompatibility and hepatic ‘first pass’ effect; reduction of side effects due to the optimization of the blood concentration-time profile; predictable and extended duration of activity; patient activated/patient modulated delivery; elimination of multiple dosing schedules, thus enhancing patient compliance; and reversibility of drug delivery by removal of drug source.13
Currently the worldwide market revenues for transdermal products are US$3 billion with an annual projected growth of 12%. Transdermal delivery systems are currently available for motion sickness, cardiovascular disease, smoking cessation, hormone replacement therapy, and pain relief (for chronic pain). According to Benson, transdermal products for cardiovascular disease, Parkinson’s disease, Alzheimer’s disease, depression, anxiety, attention deficit hyperactivity disorder (ADHD), skin cancer, female sexual dysfunction, post-menopausal bone loss, and urinary incontinence are all at various stages of formulation and clinical development.14
Benson states that “Drug molecules in contact with the skin surface can penetrate by three potential pathways: through the sweat ducts, via the hair follicles and sebaceous glands (collectively called the shunt or appendageal route), or directly across the stratum corneum. The majority of skin penetration enhancement techniques are currently being focused on increasing the transport of drugs across the stratum corneum rather than through the appendages“. The lipid-protein-partitioning theory, as developed by Barry and coworkers (1989-1991) describe the mechanisms by which enhancers effect skin permeability. These mechanisms include: disruption of the intercellular bilayer lipid structure, interaction with the intracellular proteins of the stratum corneum, and improvement of partitioning of a drug, co-enhancer, or co-solvent into the stratum corneum.
According to several research studies, essential oils, in particular terpenes, increase diffusivity of drugs within the stratum corneum by disrupting the intercellular lipid barrier and by opening new polar pathways within and across the stratum corneum. Essential oil constituents that have been found to increase dermal penetration of drugs include: Hydrocarbons: d-limonene, alpha-pinene, beta-carene; Alcohols: alpha-terpineol, terpinen-4-ol and carvol; Ketones: carvone, pulegone, piperitone, and menthone; Oxides: 1,8 cineole; and essential oils of ylang ylang, anise, and eucalyptus. Alcohols, ketones and cyclic ethers were most effective accelerants of 5-fluorouracil (a drug used in the treatment of cancer) permeation.15
I have included this information not so much because it is directly relevant to the application of aromatherapy by the average aromatherapists, but rather to gain insights into the depth of potential applications for essential oils. In relation to essential oils and the skin, research studies have shown that the application of essential oils in a gel base increases transdermal permeation and absorption of water, thereby increasing hydration in the skin.16
Aromatic Psychodermatology: The emotional role of essential oils in skincare
“The skin is the mirror which reflects the state of the mind.” is a proverb which has been used since ancient times. In the first lesson you learned that the skin shares a common origin with the nervous system and the two continue an intimate relationship throughout our lives. The skin is connected to the brain via the nervous system as well as by the endocrine and immune systems. Due to these close connections, human skin is acutely sensitive to a variety of psychological/emotional states.
Psychological stress has been shown to: exacerbate acne vulgaris17,18; disturb epidermal permeability barrier homeostasis which can lead to or exacerbate inflammatory dermatoses such as psoriasis and atopic dermatitis19; reduce epidermal cell proliferation20; and slow wound healing.21 Psychological stress, therefore, is capable of affecting many aspects of the skins function.
Psychodermatology addresses the interaction between the mind and the skin. This discipline acknowledges the complex interplay between the skin and the neuroendocrine and immune systems and has been described as the neuro-immuno-cutaneous system.22 The nervous system, endocrine system, and cutaneous immune system all cooperate to maintain the homeostasis of the skin.
According to work by Koo and Lee there are 3 main categories for psychocutaneous disorders. These include: (1)psychophysiologic disorders, (2) psychiatric disorders with dermatologic symptoms, and (3) dermatologic disorders with psychiatric symptoms.23 Let us explore these categories a bit further.
(1) Psychophysiologic disorders: In this category are skin conditions where psychiatric (emotional) factors are instrumental in the etiology and course of the skin condition. Although the skin disease is not necessarily caused by stress, stress appears to either preciptate the appearance of the condition or exacerbates it once the skin condition has appeared. Conditions falling under this category include: psoriasis, atopic dermatitis, acne excoriee (habitual act of picking at skin lesions), acne vulgaris, rosacea, alopecia areata, herpes simplex, pruritus, hyperhidrosis, and urticaria.
Stress management and relaxation techniques have been found to be quite useful when treating these skin conditions/diseases. Essential oils also have a great role to play in treating psychophysiologic disorders. As you will learn in Module 4, olfactory aromatherapy is capable of reducing the impact of stress due to its connection to the limbic/emotional region of the brain. Research on the impact of ‘aromas’ on stress-induced skin changes have shown that odorants with a sedative effect prevent the delay of skin barrier recovery induced by stress after acute barrier disruption24 and sedative odorants may be useful as a complementary therapy for atopic dermatitis through psychosomatic stress care.25 The inhalation of ‘aromas’ have also been found to affect the adrenal system via the sympathetic nervous system.26
With this in mind, essential oils considered to be relaxing, anxiety-relieving, soothing, and sedative could potentially be used to reduce the appearance or longevity of psychophysiologic disorders. The following essential oils could be used:
- Bergamot (Citrus bergamia)
- Cedarwood (Cedrus atlantica)
- Roman chamomile (Chamaemelum nobile)
- German chamomile (Matricaria recutita)
- Lavender (Lavandula angustifolia)
- Marjoram, Sweet (Origanum marjorana)
- Melissa (Melissa officinalis)
- Neroli (Citrus aurantium var. amara flos.)
- Sweet orange (Citrus sinensis)
- Petitgrain (Citrus aurantium var amara leaves)
- Rose (Rosa damascena)
- Sandalwood (Santalum album)
- Mandarin/Tangerine (red) (Citrus reticulata)
- Ylang ylang (Cananga odorata)
- Vetiver (Vetiveria zizanioides)
(2) Psychiatric disorders with dermatologic symptoms:
In this category are disorders that occur in the context of somatoform* disorders, anxiety disorder, factitious disorder, impulse-control disorder, or eating disorder.27 This is a complex category and one which will not be explored further in this section. *Somatoform disorders represent a group of disorders characterized by physical symptoms suggesting a medical disorder. However, somatoform disorders represent a psychiatric condition because the physical symptoms present in the disorder cannot be fully explained by a medical disorder, substance use, or another mental disorder.28
(3) Dermatologic disorders with psychiatric symptoms: This category includes patients who have emotional problems as a result of having a skin condition/disease. Skin conditions such as psoriasis, chronic eczema, various ichthyosiform syndromes, neurofibromas, severe acne, and disfigurement or disfiguring lesions can all have grave effects on psychosocial interactions, self-esteem, and body image. Individuals may suffer with depression, anxiety, work-related problems, low self image, social isolation, anxiety, and lack of self confidence.
Essential oils and aromatherapy have a role to play in this category of psychocutaneous disorders as well. I am reminded of a client years ago who I was blessed to work with. This female client had been in an automobile accident and as a result she had a large raised scar on the left side of her face. This scar was constantly inflamed and it bothered her a great deal. She suffered with low self esteem and depression because of it. She came to me in hopes that aromatherapy could alter the appearance of the scar tissue as well as reduce the inflammation. After an in-depth consultation, I arrived at the idea of treating the emotional aspects of the scar first while also working on changing the physical appearance of the scar.
The first blend was designed for the emotional aspects of the scar. This blend was a mix of: Rosa damascena, Boswellia carteri and Citrus reticulata. This was placed in a shea butter/jojoba base at a 4% dilution. My intent and goal was to support her in developing a different relationship with and perception of the scar. She applied the blend to her skin twice daily. We worked together for a number of months during which she did indeed arrive at another place with her scar. Over the months of applying the blend she was able to acknowledge the anger she felt over the accident. She reporting crying quite often and also feeling overwhelmed by the anger which also arose. Slowly she was able to release this anger and sadness. With this release she began to develop a different relationship with the scar. She became more accepting, more able to see the positive aspects of her life. This change in relationship with the scar reduced the inflammation. I also noticed that the scar was slowly beginning to fade although it would always be present. I realized then that sometimes it’s not about the physical manifestation but rather our emotional connection to it. It was quite an experience to watch her go through this healing process and it was an honor to help facilitate.
With this in mind, we can begin to see that essential oils have an incredible capacity to alter perceptions and relationships with dermatologic disorders with psychiatric symptoms. At times we can use essential oils to actually ‘treat’ the condition or at least treat the symptoms of the condition (e.g. reduce the inflammation of psoriasis or eczema) and at other times we can utilize essential oils to facilitate different relationships to or perceptions of the disfigurement or skin condition in hopes that this will lead to a better quality of life and a better sense of self.
Aromatherapy is by no means a panacea nor does it work on this level without a degree of willingness and full participation on behalf of the client. However, the potential is great and aromatherapy is at times quite extraordinary in the manner in which it can affect people. In Module Four you will explore olfactory aromatherapy further. My hope is that this opens doors and ideas for unique applications of essential oils for the relief and treatment of psychocutaneous disorders.
To conclude this lesson we shall now turn to safety and essential oils. Please note: This section is a review of information contained within the School for Aromatic Studies ‘Foundations of Aromatherapy’ course.
Safety and Essential Oils
Safety involves a state of being free from risk or occurrence of injury, harm, or danger. Individuals who practice aromatherapy need to be aware of the safety issues involved with using essential oils in order to avoid potential adverse effects. According to Burfield, “Although many essential oils are potentially hazardous materials, if handled in the appropriate manner, the risks involved in their use can be very small. So therefore, most commercially offered essential oils are safe to use for the purpose intended in a domestic/professional or clinical environment”.29 Schnaubelt states that the “informed use of essential oils may create occasional irritation or minor discomfort, but it is extremely unlikely to create serious injury or lasting physical problems,”30 particularly when basic guidelines are followed.
Factors which influence the safety of essential oils include:
1. Quality of essential oil being utilized: Adulterated essential oils increase the likelihood of an adverse response and hence the need for pure, authentic, and genuine essential oils is of the utmost importance. This point cannot be overstated.
2. Chemical composition of the oil: Essential oils rich in aldehydes (e.g., citronellal, citral) and phenols (e.g., cinnamic aldehyde, eugenol) may cause skin reactions. Oils rich in these constituents should always be diluted prior to application to the skin. According to Schnaubelt, “diluting such oils so that the resulting solution becomes non-irritant, may require diluting them to concentrations much lower than in normal circumstances. Another option is to blend such irritant oils asymmetrically with other essential oils, which mitigate their irritant effects”.31
3. Method of application: Essential oils may be applied on the skin (dermally), inhaled, or taken internally. The potential safety concerns with dermal application will be discussed below. With regard to inhalation, Tisserand and Balacs state: “Inhalation, from a safety standpoint, presents a very low level of risk to most people. Even in a relatively small closed room, and assuming 100% evaporation, the concentration of any essential oil (or component thereof) is unlikely to reach a dangerous level, either from aromatherapy massage, or from essential oil vaporization”.32 They further point out that “the only likely risk would be from prolonged exposure (perhaps 1 hour or more) to relatively high levels of essential oil vapor which could lead to headaches, vertigo, nausea and lethargy”.
With regard to internal use, this method of application is not discussed in this textbook and further training is recommended prior to using essential oils internally.
4. Dosage/dilution to be applied: Most aromatherapy blends for massage and bodywork will be between 1 and 5 percent dilutions, which typically does not represent a safety concern. As one increases dilution, potential dermal (skin) reactions may take place depending on the individual essential oil, the area in which the oil is applied, and other factors related to the client’s own sensitivity levels. Schnaubelt comments: “Any excessive usage of essential oils may cause irritation or other undesired effects due to their lipophilic nature”.33
5. Integrity of skin: Damaged, diseased, or inflamed skin is often more permeable to essential oils and may be more sensitive to dermal reactions. According to Tisserand and Balacs, “It is potentially dangerous to put undiluted essential oils on to damaged, diseased or inflamed skin. Under these circumstances the skin condition may be worsened, and larger amounts of oil than normal will be absorbed. Sensitization reactions are also more likely to occur”.34
Possible Dermal Reactions
Of primary concern to those applying essential oils to the skin are possible dermal reactions. According to Tisserand and Balacs, “skin reactions take three forms: irritation, sensitization and phototoxicity”.35
Dermal irritant
A dermal irritant will produce an immediate effect of irritation on the skin. The reaction will be represented on the skin as blotchy or redness, which may be painful to some individuals. Irritant reactions to essential oils can be divided into severe, strong, moderate, or weak. According to Bensouilah and Buck, “strong irritants are capable of provoking visible skin damage after just a single exposure, whereas weak irritants require frequent multiple exposures over months or even years to produce cumulative or chronic irritant contact dermatitis”.36 The severity of the reaction will depend on the essential oil and its chemical makeup, the concentration (dilution) applied and the sensitivity of the skin to which it is applied.
General safety guidelines include: avoid application of known dermal irritant essential oils on any inflammatory or allergic skin condition; avoid undiluted application; avoid application on open or damaged skin; and dilute known dermal irritants with appropriate vegetable oil or other carrier. Essential oils rich in aldehydes or phenols are the most likely candidates for dermal irritation. It is recommended that essential oils rich in these components not exceed 20% of a formulation for use in up to 15% concentrations.37
Should irritation occur wipe off the blend quickly by using an absorbent tissue or cloth then apply a vegetable oil or unscented cream to the affected area. Remove the vegetable oil or cream with absorbent tissue then reapply vegetable oil or cream. Repeat this process 4-5 times. Do not use water or soap on the irritated area as this may lead to further irritation.38
Bensouilah and Buck recommend that when one is formulating, in order to avoid skin irritancy always consider the following:
- Potential irritancy of each oil (is it rich in aldehydes or phenols)
- Potential irritancy of combined oils (ditto)
- Total aldehyde and phenol concentration in final product
- Site and surface area to which the formulation will be applied
- Skin integrity
- Disorder being treated
- Age (older mature skin is thinner and can be more sensitive) and skin type
Please remember: Irritation reactions are limited to site of application and any irritation which occurs will fade quickly once the irritant is removed. Table 1.1 outlines common essential oils that may cause dermal irritation.
| Table 1.1 Dermal Irritants | |
|---|---|
| Essential Oil | Latin Name |
| Bay | Pimento racemosa |
| Cinnamon bark or leaf | Cinnamomum zeylanicum (Bark is more irritating than leaf) |
| Clove bud | Syzygium aromaticum |
| Citronella | Cymbopogon nardus |
| Cumin | Cuminum cyminum |
| Lemongrass | Cymbopogon citratus |
| Lemon verbena | Lippia citriodora syn. Aloysia triphylla |
| Oregano | Origanum vulgare |
| Tagetes | Tagetes minuta |
| Thyme ct. thymol | Thymus vulgaris |
| All citrus oils have the potential to be skin irritants if used in high dosages. | |
Dermal Sensitization
Dermal sensitization is a type of allergic reaction. It occurs on first exposure to a substance, but on this occasion, the noticeable effect on the skin will be slight or absent. However, subsequent exposure to the same material, or to a similar one with which there is cross-sensitization, produces a severe inflammatory reaction brought about by cells of the immune system (T-lymphocytes).39 The reaction will be represented on the skin as blotchy or redness, which may be painful to some individuals.
The problem with dermal sensitization is that once it occurs with a specific essential oil the individual is most likely going to be sensitive to it for many years and perhaps for the remainder of his/her life. The best way to prevent sensitization is to avoid known dermal sensitizers and avoid applying the same essential oils every day for lengthy periods of time. Sensitization is, to an extent, unpredictable, as some individuals will be sensitive to a potential allergen and some will not.40
According to Burfield, the following oils listed in Table 1.2 are considered to be dermal sensitizers and are not recommended for use in aromatherapy massage.41
| Table 1.2 Dermal Sensitizers | |
|---|---|
| Essential Oil | Latin Name |
| Casia | Cinnamomum cassia |
| Cinnamon bark | Cinnamomum zeylanicum |
| Clove leaf (moderate) | Eugenia caryophyllata |
| Peru balsam | Myroxylon pereirae |
| Verbena absolute (moderate) | Lippia citriodora |
| Absolutes of: oakmoss, treemoss, lavender, and lavandin | |
| Turpentine oil | Pinus spp. |
| Backhousia | Backhousia citriodora |
| Oxidized oils from Pinaceae family (e.g., Pinus and Cupressus species) and Rutaceae family (e.g., citrus oils) - low risk | |
Photosensitization
An essential oil that exhibits this quality will cause burning or skin pigmentation changes, such as tanning, on exposure to sun or similar light (ultraviolet rays). Reactions can range from a mild color change through to deep weeping burns. Do not use or recommend the use of photosensitizing essential oils prior to going into a sun tanning booth or the sun. Recommend that the client stays out of the sun or sun tanning booth for at least twenty-four hours after treatment if photosensitizing essential oils were applied to the skin. Certain drugs, such as tetracycline, increase the photosensitivity of the skin, thus increasing the harmful effects of photosensitizing essential oils under the necessary conditions. Table 1.3 lists some common essential oils considered to be photosensitizers. Table 1.4 lists citrus essential oils that are not considered to be phototoxic.
| Table 1.3 Photosensitizers | |
|---|---|
| Essential oil | Latin name |
| Angelica root | Angelica archangelica |
| Bergamot | Citrus bergamia |
| Cumin | Cuminum cyminum |
| Distilled or Expressed Grapefruit (low risk) | Citrus paradisi |
| Expressed Lemon | Citrus limon |
| Expressed Lime | Citrus x aurantifolia or Citrus x latifolia |
| Expressed Bitter Orange | Citrus aurantium |
| Rue | Ruta graveolens |
| Table 1.4 Non-phototoxic citrus oils | |
|---|---|
| Essential Oil | Latin Name |
| Bergamot: Bergapteneless (FCF: Furanocoumarin Free) | Citrus bergamia |
| Distilled lemon | Citrus limon |
| Distilled lime | Citrus x aurantifolia or Citrus x latifolia |
| Mandarin/Tangerine | Citrus reticulata |
| Sweet orange | Citrus sinensis |
| Expressed tangerine | Citrus reticulata |
| Yuzu (expressed or distilled) | Citrus juno |

Idiosyncratic irritation or sensitization
Idiosyncratic irritation or sensitization is an uncharacteristic or unusual reaction to a commonly used essential oil. This type of reaction is difficult to predict and rarely occurs but is a possibility.
Mucous membrane irritant
A mucous membrane irritant will produce a heating or drying effect on the mucous membranes of the mouth, eyes, nose, and reproductive organs. It is recommended that mucus membrane irritating essential oils not be used in a full body bath unless placed in a dispersant first (e.g., milk, vegetable oil). Bay, clove, cinnamon bark, lemongrass, and thyme ct. thymol essential oils should be avoided in baths completely. Table 1.5 lists some common essential oils considered to be mucous membrane irritants.
| Table 1.5 Mucous membrane irritants | |
|---|---|
| Essential Oil | Latin Name |
| Bay | Pimento racemosa |
| Caraway | Carum carvi |
| Cinnamon bark or leaf | Cinnamomum zeylanicum |
| Clove bud or leaf | Syzygium aromaticum |
| Lemongrass | Cymbopogon citratus |
| Peppermint | Mentha x piperita |
| Thyme ct. thymol | Thymus vulgaris |
Additional Reading:
- Read about how German chamomile essential oil in a gel base acts as a penetration enhancer for water: hydrationgchamresearch-1
- Read AntiDermatophytic activity of Essential Oils






